Question 1
What is the favoured hand-washing strategy in order to prevent intravascular catheter associated infections?
(A) providone-iodine alcohol
(B) chlorhexidine-alcohol
(C) lux soap
(D) hypertonic saline
(E) isopropyl alcohol
B: According to a recent landmark multi centre randomised trial published by the CLEAN investigators, chlorhexidine-alcohol is superior to provide-iodine alcohol (0·28 vs 1·77 per 1000 catheter-days with povidone iodine–alcohol; hazard ratio 0·15, 95% CI 0·05–0·41; p=0·0002) Lancet 2015; 386(1008) 2069 - 2077
Question 2
After S. aureus, what is the second most implicated organism in vertebral osteomyelitis?
(A) S. epidermis
(B) S. viridian's
(C) Enterococci faecalis
(D) E. Coli
(E) N. Gonorrhoea
D: S. aureus is the most common bacterial pathogen, however in acute vertebral osteomyelitis, E. Coli is the second most implicated organism. Vertebral osteomyelitis often occurs through haematogenous seeding rather than from direct seeding. Coagulase-negative staphylococci and Propionibacterium acnes are the microorganisms that are almost always the cause of exogenous osteomyelitis after spinal surgery, particularly if fixation devices are used. The primary source of infection has been identified as urinary tract, skin, or soft tissue; a site of vascular access; or endocarditis, bursitis, or septic arthritis. Clin Infect Dis 2002;34:1342-1350; ; N Engl J Med 2010; 362:1022-1029
Question 3
What is the most sensitive imaging modality used to investigate vertebral osteomyelitis?
(A) Plain X-ray
(B) CT scan
(C) MRI scan
(D) PET-CT
(E) Bone scan
C: By far, highest sensitivity is for MRI scans. Features of imaging include end plate erosions, disc oedema (T2 images), inflammatory phlegmon. It also enables differentiation from other alternative causes, such as metastatic deposits, disc herniation etc and may be able to show evidence of paravertebral abscess and epidural abscess. Typically, the disk space and two adjacent vertebral bodies are involved. Reported accuracy of Bone scan is 67%. Positron-emission tomographic (PET) scanning with 18F-fluorodeoxyglucose has a diagnostic accuracy similar to that of MRI and may be a better choice when the patient has metallic implants. However, experience with this practice is still limited. Best Pract Res Clin Rheumatol 2006;20:1197-1218, N Engl J Med 2010; 362:1022-1029, Clin Nucl Med2000;25:963-977, Semin Musculoskelet Radiol 2007;11:353-364
Question 4
At which location is vertebral osteomyelitis more likely to present?
(A) lumbar spine
(B) cervical spine
(C) thoracic spine
(D) sacrum
(E) atlas
A: The lumbar spine is the most common site of presentation of vertebral osteomyelitis.
Question 5
A 71 year old lady presents with neck pain on a background of severe osteoporosis. She does not note any recent history of trauma. She had previously suffered from post-polio syndrome, and required the insertion of fixation rods to her right leg 10 years ago. She is also colonised with MRSA. During her fixation, her inpatient stay was complicated by an enterobacter wound infection. She has been taking ciprofloxacin life long. Her MRI of her neck is shown below (image from radiopedia.org)
What is the favoured hand-washing strategy in order to prevent intravascular catheter associated infections?
(A) providone-iodine alcohol
(B) chlorhexidine-alcohol
(C) lux soap
(D) hypertonic saline
(E) isopropyl alcohol
B: According to a recent landmark multi centre randomised trial published by the CLEAN investigators, chlorhexidine-alcohol is superior to provide-iodine alcohol (0·28 vs 1·77 per 1000 catheter-days with povidone iodine–alcohol; hazard ratio 0·15, 95% CI 0·05–0·41; p=0·0002) Lancet 2015; 386(1008) 2069 - 2077
Question 2
After S. aureus, what is the second most implicated organism in vertebral osteomyelitis?
(A) S. epidermis
(B) S. viridian's
(C) Enterococci faecalis
(D) E. Coli
(E) N. Gonorrhoea
D: S. aureus is the most common bacterial pathogen, however in acute vertebral osteomyelitis, E. Coli is the second most implicated organism. Vertebral osteomyelitis often occurs through haematogenous seeding rather than from direct seeding. Coagulase-negative staphylococci and Propionibacterium acnes are the microorganisms that are almost always the cause of exogenous osteomyelitis after spinal surgery, particularly if fixation devices are used. The primary source of infection has been identified as urinary tract, skin, or soft tissue; a site of vascular access; or endocarditis, bursitis, or septic arthritis. Clin Infect Dis 2002;34:1342-1350; ; N Engl J Med 2010; 362:1022-1029
Question 3
What is the most sensitive imaging modality used to investigate vertebral osteomyelitis?
(A) Plain X-ray
(B) CT scan
(C) MRI scan
(D) PET-CT
(E) Bone scan
C: By far, highest sensitivity is for MRI scans. Features of imaging include end plate erosions, disc oedema (T2 images), inflammatory phlegmon. It also enables differentiation from other alternative causes, such as metastatic deposits, disc herniation etc and may be able to show evidence of paravertebral abscess and epidural abscess. Typically, the disk space and two adjacent vertebral bodies are involved. Reported accuracy of Bone scan is 67%. Positron-emission tomographic (PET) scanning with 18F-fluorodeoxyglucose has a diagnostic accuracy similar to that of MRI and may be a better choice when the patient has metallic implants. However, experience with this practice is still limited. Best Pract Res Clin Rheumatol 2006;20:1197-1218, N Engl J Med 2010; 362:1022-1029, Clin Nucl Med2000;25:963-977, Semin Musculoskelet Radiol 2007;11:353-364
Question 4
At which location is vertebral osteomyelitis more likely to present?
(A) lumbar spine
(B) cervical spine
(C) thoracic spine
(D) sacrum
(E) atlas
A: The lumbar spine is the most common site of presentation of vertebral osteomyelitis.
Question 5
A 71 year old lady presents with neck pain on a background of severe osteoporosis. She does not note any recent history of trauma. She had previously suffered from post-polio syndrome, and required the insertion of fixation rods to her right leg 10 years ago. She is also colonised with MRSA. During her fixation, her inpatient stay was complicated by an enterobacter wound infection. She has been taking ciprofloxacin life long. Her MRI of her neck is shown below (image from radiopedia.org)
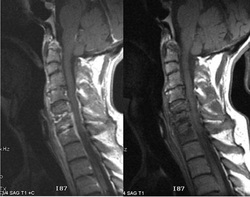
What is the best management approach for this lady?
(A) immediate antibiotics with vancomycin and broad gram negative coverage
(B) immediate neurosurgical consultation, multiple repeat blood cultures and if negative an image guided bone biopsy
(C) Discharge for out-patient follow-up with progress MRI
(D) immediate neurosurgical consultation with prompt initiation of antibiotics
(E) Radiotherapy
B: Vertebral osteomyelitis without spinal cord compression is not an acute microbiological emergency. Whilst neurosurgical intervention should be promptly ascertained, it is imperative to obtain a microbiological diagnosis. This is even more important in this case as she has been on treatment with ciprofloxacin. The clinical practice article in NEJM suggested that if antibiotics have already been initiated and there is no clinical urgency then antibiotics may be ceased for 48 hours whilst cultures and further investigations are being undertaken. " In a systematic review of studies of vertebral osteomyelitis, positive blood cultures were reported in 58% of the cases (range across studies, 30 to 78%). If vertebral osteomyelitis is suspected after imaging is performed (see below) and blood cultures do not show growth of microorganisms, a biopsy is generally warranted" N Engl J Med 2010; 362:1022-1029, Semin Arthritis Rheum2009;39:10-17
Question 6
A 43 year old male presents with 3 weeks of fevers and weight loss. Examination reveals an early diastolic murmur over the aortic region. A TTE shows an oscillating vegetation over the aortic valve. Blood cultures subsequently confirm a S. bovis bacteremia. He successfully completes a prolonged course of antibiotics for infective endocarditis. The JMO, in his eager role to please the consultant, discharges him thinking the patient is safe. Where did he go wrong?
(A) He forgot to order a repeat TTE
(B) He forgot to ensure valvular anatomy with TOE
(C) He forgot to rule out malignant or pre-malignancy with a colonoscopy
(D) He forgot to discharge the patient on oral antibiotics as prophylaxis
(E) He did the right thing
C: S. bovis bacteraemia, with or without endocarditis is associated with colorectal pre malignancy or malignancy Arch Intern Med. 1978;138(7):1097-9.
Question 7
A 46 year old male with HIV presents with an occulomotor cranial nerve palsy, headache with stiff neck and a diffuse macular papular rash. Examination of the anal region reveals the following picture (bmj.com)

What is the most likely diagnosis?
(A) Primary syphillis
(B) Secondary Syphilis
(C) Early Latent syphilis
(D) Late latent syphilis
(E) Neurosyphilis
B: This patient has the classic manifestation of secondary syphilis, with cranial nerve palsies, an aseptic meningitis, classic rash and condylomata lata. Secondary syphilis occurs when the spirochetes achieve a bacteraemia and distribute to end organs. Primary syphilis occurs after primary infection and is most classically described as a chancre, which is a painless ulcer at the site of inoculation. Primary syphilis regresses and secondary syhilis subsequently develops. Following secondary syphilis tertiary syphilis develops. An arbitrary time point of 2 years post infection differentiates early latent from late latent syphilis. The distinction is important as it determines treatment response. Neurosyphilis is a type of tertiary syphilis and is characterised by a psychotic-demeting syndrome or tabes dorsalis - ataxic syndrome. Other manifestations of syphilis include cardiovascular sphilis which is characterised by aortitis and gumma - granulomatous reactions to spirochetes which commonly involve the bone and skin. Treatment is usually with benzylpenicillin, although azithromycin and doxycycline can be used. Pregnant females must be treated with benzylpenicillin and if they have a type 1 hypersensitivity reaction they must be desensitised to the penicillin. BMJ 2007;334:143
Question 8
A 46 year old male presents with a primary chancre like lesion. The medical registrar takes a swab and sends it of for culture. What is TRUE regarding the diagnosis of primary syphilis in this particular case?
(A) Culture results are available within 1 week
(B) Culture results take at least 1 month to become positive
(C) Culture of T. pallidum is not possible and thus diagnosis is based upon serology and/ or direct visualisation of motile spirochetes in normal saline when examined through dark field microscopy
(D) Culture results take 1 week, sensitivities will take 1 month
(E) Clinical diangosis of T. pallidum is the gold standard as serology, culture and direct visualisation are all insensitive tools
C: Diagnosis can be made via direct visualisation, treponemal specific (TPHA/ TPPA/ ELISA) tests and nontreponemal tests (VRDL = RPR). The nontreponemal tests are traditionally used as part of primary screening, and the treponemal tests are used as confirmatory tests. The non treponemal tests use an indirect method of reactivity of patient serum against cardiolipin-cholesterol-lecithin antigen. Postive tests are reported as a titre, and titres decrease over time with treatment (they decrease much slower without treatment). BMJ 2007;334:143
Question 9
What type of organism is Salmonella enteric serotype typhi?
(A) Gram positive cocci
(B) Gram positive bacilli
(C) Gram negative cocci
(D) Gram negative cocco-bacilli
(E) Gram negative bacilli
E. BMJ 333(7558), 78 – 82
Question 10
What is the maximum incubation period for enteric fever?
(A) 4 days
(B) 2 weeks
(C) 20 days
(D) 1 month
(E) 2 months
E: BMJ 333(7558), 78 – 82
Question 11
For what illness does the step-ladder fever apply to?
(A) Enteric fever
(B) Dengue fever
(C) Malaria
(D) Hepatitis A
(E) HIV
A: The step-ladder fever describes a fever that progressively increases in amplitude followed by a plateau period and subsequent decline to baseline. Classically the increase is over one week, followed by a plateau of one week and then a subsequent decrease to baseline over one week. BMJ 333(7558), 78 – 82
Question 12
Which of the following agents does NOT have in vivo activity against S. enterica serotype typhi?
(A) Gentamicin
(B) Chloramphenicol
(C) Azithromycin
(D) Ceftriaxone
(E) Ciprofloxacin
A. Whilst there is in vitro activity, gentamicin does not have in vivo activity. The same statement applies to first and second generation cephalosporins. The treatment of enteric fever is complicated as resistance patterns changes. Fluroquinolones are the best option if there is demonstrated susceptibility. Chloramphenicol has a black-box warning of causing agranulocytocis. Azithromycin is an effective agent and can be used orally, as can the third generation cephalosporins. Cochrane Database of Systematic Reviews (2), CD004530
Question 13
A 45 year old male who returned from Thailand 4 weeks ago presents with a transient maculopapular rash, fevers, headaches, abdominal pain, constipation, clinical splenomegaly and blood cultures demonstrating gram negative cocci. An abdominal ultrasound shows gallbladder wall thickening. He is febrile but with a relative bradycardia. Blood cultures demonstrate gram negative bacilli. Thick and thin films are negative for malaria. With regards to the most likely diagnosis, what is the correct practice in terms of isolation practices in a tertiary centre?
(A) no contact precautions, no isolation
(B) contact precautions but no isolation
(C) contact precautions, isolation, positive pressure room
(D) contact precautions, isolation, negative pressure room
(E) contact precautions, isolation, normal single room
E: This is likely enteric fever caused by S. typi/ paratyphi. This is a notifiable disease and transmission is through the faecal-oral route. In addition, there is no animal vector for these specific serotypes, thus spread is purely human to human. The patient should be in isolation with contact precautions until stool cultures have cleared. Australian and New Zealand Journal of Public Health 25(6), 539 – 542
Question 14
Ecthyma gangrenosum is found in what bacterial infection?
(A) Vibrio vulnificus
(B) Streptococcus pyogenes
(C) Staphylococcus epidermidis
(D) Staphylococcus aureus
(E) Pseudomonas aureginosa
E: Found in neutropenic sepsis with pseudomonas bacterial emboli to skin. PEP 2014
Question 15
A 36 year old female from Gungahlin, Canberra presents with spreading cellulitis following a cat bite. Which of the following antibiotics should be used?
(A) Vancomycin
(B) Flucloxacilin
(C) Cephazolin
(D) Clindamycin
(E) Amoxicilin
E: Cat bite puts this patient at risk of Pasturella infection. Pasteurella multocida is sensitive to amoxicillin, penicillins and doycycline, but resistant to the other antibiotics. This organism is found as part of the normal flora of cats and dogs, and is a gram negative coccobacilli. Am Fam Physician 90: 239, 2014
Question 16
A 29 year old female has been trekking through the daintree rainforest over one month ago. She subsequently presents with an ulcer that has been growing slowly but with a siginficantly deep ulcer base. What is the most likely bacterial aetiology?
(A) Mycobacterium ulcerans
(B) Mycoplasma hominis
(C) Staphylococcus aeureus
(D) Mycobacterium abscessus
(E) Mycobaterium avium complex
A: Also known as the buruli ulcer. It is a slowly progressive destructive infection of skin and of adipose and soft tissue caused by Mycobacterium ulcerans, an environmental pathogen that produces a potent toxin. It is particularly endemic to coastal victoria and the daintree region. Med J Aust 2014; 200 (5): 267-270.
Question 17
The New dehli metalo-betalactamase is resistant to all antimicrobials apart from:
(A) Colistin (polymixin)
(B) Vancomycin
(C) Daptomycin
(D) Meropenem
(E) Ceftaroline
A:
- · Transmissible genetic component encoding multiple resistance genes (additional resistance mechanisms in addition to carbapenemase)
- · Isolated from strain of Klebsiella from a patient who acquired organism in New Delhi
- · Described now in Klebsiella, E. Coli and enterobacter
- · Subsequently organisms in the Enterobacteriaceae family containing this genetic element have been found widely throughout the world. Initially India, Pakistan and Bangladesh, now Aus, UK, Europe and Asia
- · Resistant to all antimicrobial agents except the polymycins (colistin)
- · Easily transferred to other Enterobacteriacea
- · Global dissemination
Question 18
Meropenem is a carbapenem that has extended spectrum activity, covering many classes of bacteria. Which two important nosocomial bacteria does meropenum have no activity against?
(A) Burkholderia cepacia and Stenotrophomonas maltophilia
(B) P. aeruginosa and enterobacter
(C) Citrobacter and Proteus
(D) Serratia and E. Coli
(E) Klebsiella and Methicillin sensitive S. Aureus
A - PEP 2014
Question 19
What is FALSE about monobactams?
(A) Aztreonam has a place in patients who have anaphylaxis to penicillins
(B) Aztreonam has activity against Gram negative organisms of similar coverage to aminoglycosides
(C) Aztreonam has activity against ESCAPPM organisms
(D) Aztreonam has activity against Pseudomonas spp
(E) Aztreonam has broad gram positive activity
E: PEP lecture . Aztreonam is the only drug in this class
- Equivalent to gentamicin with regards to gram negative cover
- It is notable since it has good activity against Gram-negative pathogens but is inactive against gram positive organisms and anaerobes
- It is of limited value only against ‘ESCAPPM’ organisms.
- Aztreonam’s main claim to fame is that for patients with severe penicillin allergy it can be used with minimal risk of cross-reactivity
- Overall, however there is little role for aztreonam therapeutically (may be used in CSF patients for Pseudomonas)
Question 20
Teicoplanin is an example of what class of antibiotics?
(A) Aminoglycoside
(B) Beta-lactam
(C) Fluroquinolone
(D) Glycopeptide
(E) Macrolide
D: Vancomycin and teicoplanin are examples of glycopeptides. These bind to the D-ala-D-ala moiety on the peptidoglycan cell wall and thus inhibit the action of the penicillin binding proteins. Enterococcus has evolved VanA --> Van G, VanA being the most common, which is a mobile genetic element that is able to change the D-ala-D-ala moiety to D-ala-D-lac. Clin Microbiol Rev. 2000 Oct; 13(4): 686–707. The most common adverse effect of teicoplanin is thrombocytopenia. Vancomycin and teicoplanin are alternatives to ampicillin or penicillin for the treatment of serious enterococcal infections where they are usually combined with an aminoglycoside to obtain antibacterial synergy. RAP Course 2015, PEP 2014
Question 21
Burkholderia cepacia, when isolated from the lungs of patients with cystic fibrosis, is a significant pathogen with much morbidity and mortality and can cause a cavitating pneumonia. What type of organism is it?
(A) Gram positive bacilli
(B) Gram negative bacilli
(C) Gram positive cocci
(D) Gram negative cocci
(E) Gram negative cocco-bacilli
B: Infections occur in the setting of immunocompromised hosts and healthcare-associated infections, and is an important pulmonary pathogen in patients with cystic fibrosis. Unfortunately there is a paucity of high-quality clinical studies to help in antimicrobial therapy in this condition. NEJM 367:2171, 2012; Syst Appl Microbiol 34: 87, 2011
Question 22
With regards to vancomycin, what is the most important pharmacodynamic principle that governs its efficacy with regards to its antimicrobial mechanism?
(A) Peak concentration reached
(B) Time spent above the minimum inhibitory concentration
(C) Area under the concentration curve divided by MIC
(D) Elimination half life
(E) Degree of protein binding
C: Peak concentration reached is important for antimicrobials such as fluroquinolones and aminoglycosides. Time spent above the MIC is important for beta lactams and AUC/ MIC is the guiding principle with regards to dose of vancomycin. Clin Infect Dis. (2006) 42(Supplement 1): S35-S39.doi: 10.1086/491712
Question 23
Which of the following antimicrobials does NOT belong to the aminoglycoside class
(A) Gentamicin
(B) Daptomicin
(C) Streptomicin
(D) Amikacin
(E) Tobramycin
B: Daptomycin is a lipopeptide that has mainly gram positive activity, and is particularly useful against MRSA and VRE. Its mechanism of action is unique - the antimicrobial itself inserts into the cell membrane, disrupting function, increasing permeability to ions, causing membrane depolarisation and ultimately disruption of protein function. It is inacitvated by pulmonary surfactant and as such can not be used in the treatment of respiratory infections. NEJM 355: 653, 2006
Question 24
Which of the following is NOT a contraindication to the use of aminoglycosides?
(A) myaesthenia gravis
(B) previous vestibular toxicity relating to gentamicin use
(C) previous cochlear toxicity relating to gentamicin use
(D) Guillian-barre syndrome
(E) Previous hypersensitivty reaction to gentamicin use
D: Aminoglycosides such as gentamicin partially block the neuromuscular junction and dramatically worsen myasthenia gravis Aust Prescr 2007;30:156-60
Question 25
Which of the following therepeutic drug monitoring principles should be used to guide gentamicin dosing in patients with infective endocarditis treatment?
(A) AUC calculations
(B) Peak concentrations
(C) Troph concentrations
(D) Random time-point concentrations
(E) 6 hours post administration concentration
C: In patients with multiple daily (synergistic dosing), therepeutic monitoring guidelines suggest that troph concentrations should be monitored twice weekly Intern Med J 2011;41(6):441-9
Question 26
Which of the following therepeutic drug monitoring principles should be used to guide gentamicin dosing in patients undergoing once daily extended treatment regimes.
(A) AUC calculations
(B) Peak concentrations
(C) Troph concentrations
(D) Random time-point concentrations
(E) 6 hours post administration concentration
A: The therapeutic guidelines suggest using AUC calculations, which are computed based on computer programs (ALLADIN in Australia). To calculate the AUC, the aminoglycoside plasma concentration needs to be obtained at two time points after drug dosing (usually 5 minutes after completion of the infusion, and 6 to 8 hours postdose). A computer program is used to calculate the AUC, which is then used to estimate the appropriate subsequent aminoglycoside dose. For once-daily or less frequent dosing, achieving an adequate area under the concentration–time curve (AUC) of aminoglycoside, while having an undetectable trough (predose) plasma concentration, is associated with clinical efficacy and minimises toxicity. Intern Med J 2013;43(5):519-25
Question 27
Linezolid is a relatively new antimicrobial. What is the mechanism of action?
(A) Inhibits DNA gyrase
(B) Inhibits the 50S ribosomal subunit
(C) Inhibits the 30S ribosomal subunit
(D) Inhibits cross-linking of the cell wall
(E) Inhibits the action of the penicillin binding protein
B: RPA Lectures 2016
Question 28
A 46 year old male presents with myoclonus, fevers, rigidity and confusion. He was on Linezolid for the treatment of a multi-resistant MRSA soft tissue infection on the wards. He has a past medical history of poorly controlled depression, COPD, ischaemic heart disease and renal impairment. He had a run of asymptomatic atrial fibrillation with rapid ventricular response rate. Which of the following medications that were recently added may have contributed to his presentation.
(A) warfarin
(B) salbutamol nebs
(C) fluoxetine
(D) amlodipine
(E) verapamil
C: Linezolid is a reversible MAO inhibitor therefore co-administration of a serotonergic agent may trigger a serotonin syndrome. It has 100% oral bioavailability and there is no renal adjustment that is made. It is active against most gram positive agents including enterococcus, MRSA, streptococci. Myelosupression, optic and peripheral neuropathy are also toxicities of this medication. It cannot clear a bacteraemia.
Question 29
Dr JM is a general physician in a peripheral hospital looking after a patient with severe cavitating pneumonia. Unfortunately the patient is colonised with MRSA. He is treated with daptomycin but unfortunately the patient died within 14 hours. A morbidity and mortality meeting was held and a discussion was made regarding appropriate antimicrobial prescribing. What is true with regards to the use of daptomycin in this particular case
(A) Daptomycin was indicated as it has activity against MRSA (and VRE)
(B) The patient died because of daptomycin related toxicity
(C) Daptomycin should not be used in pneumonia as it is inactivated by pulmonary surfactant
(D) Daptomycin is inactive against MRSA (and VRE)
(E) Daptomycin was likely to have interacted with CYP substrates that the patient was already taking
C. Daptomycin is predominantly excreted unchanged in the kidneys, with no hepatic metabolism. Toxicity includes myopathy and an eosinophilic pneumonia. It can also cause a falsely prolonged INR with no anticoagulation effect.
Question 30
What is the most common cause of severe sepsis?
(A) Pneumonia
(B) Urosepsis
(C) Intra-abdominal sepsis
(D) Sepsis related to in-dwelling lines
(E) Soft tissue infections
A: Pneumonia is the most common cause, accounting for about half of all cases, followed by intraabdominal and urinary tract infections. N Engl J Med 2013; 369:840-851
