- Nicotine is highly addictive substance: Essentially it signals via the central nicotinic receptors in the ventral tegmental area --> nucleus accumbens --> prefrontal cortex via dopamine release, crucial in reward pathways
- Therefore tobacco uses aim to maintain steady state of nicotine concentration in blood - prevent withdrawal, maintain pleasure/ arousal/ modulate mood
- Users self titrate by taking more frequent ciggs/ smoke more intensely (deeper breaths)
- A 2 pronged problem - should therefore look at both these aspects
- Physiological effects of nicotine on reward pathways
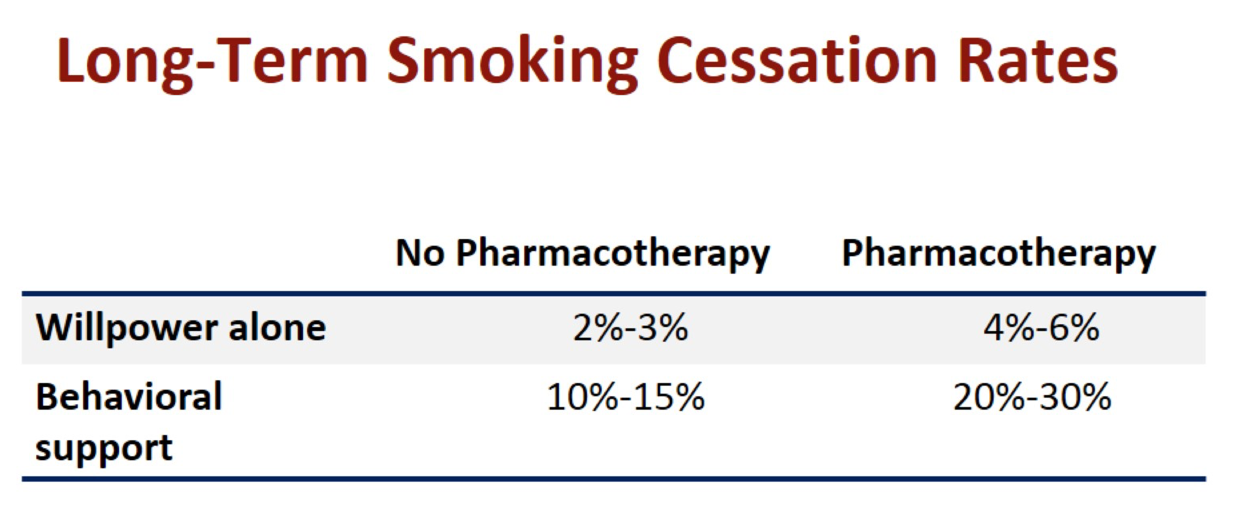
- Behavioural aspects of addiction --> behavioural therapies
- Pharmacological treatment
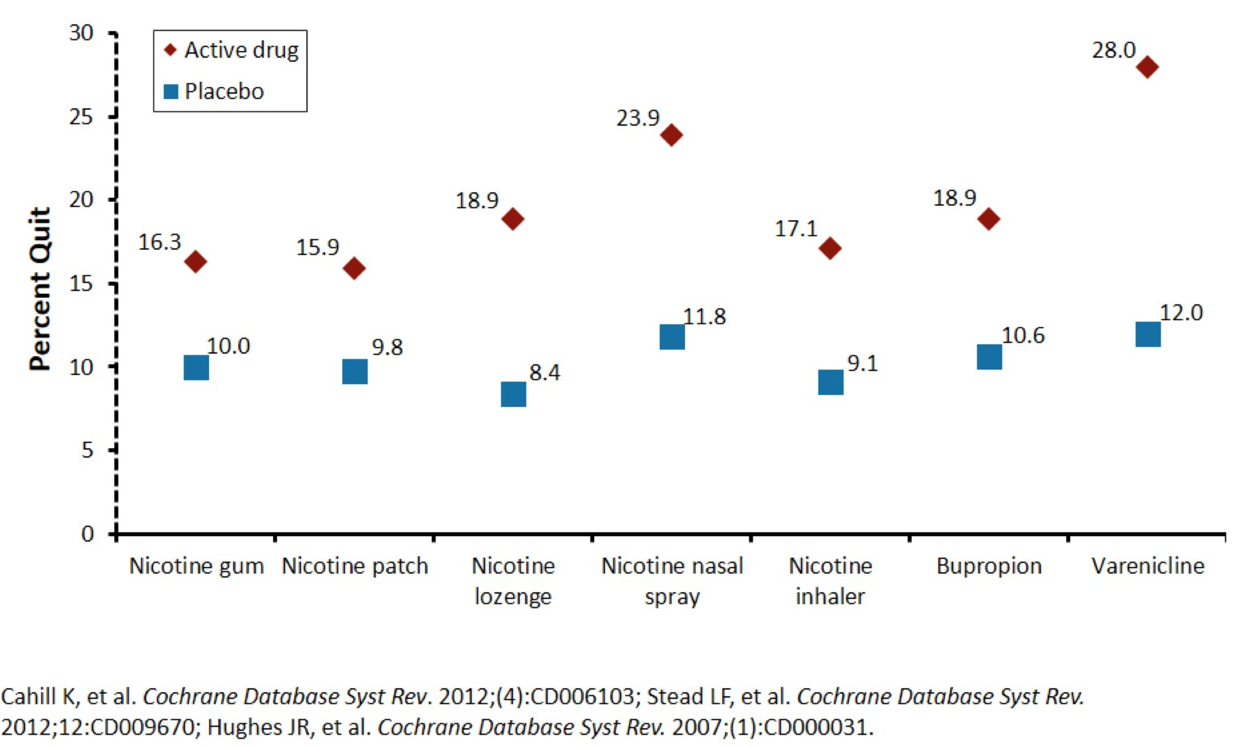
- NRT
- partial nicotine receptor agonists
- varenicline
- cytisine
- psychotropics
- sustained release bupropion
- Information regarding trials in smoking cessation
- patients recruited tend to be more motivated, cognitive therapy tends to be more intensive
- Drug treatment only trialled for 12 weeks, but dependency is a chronic disease
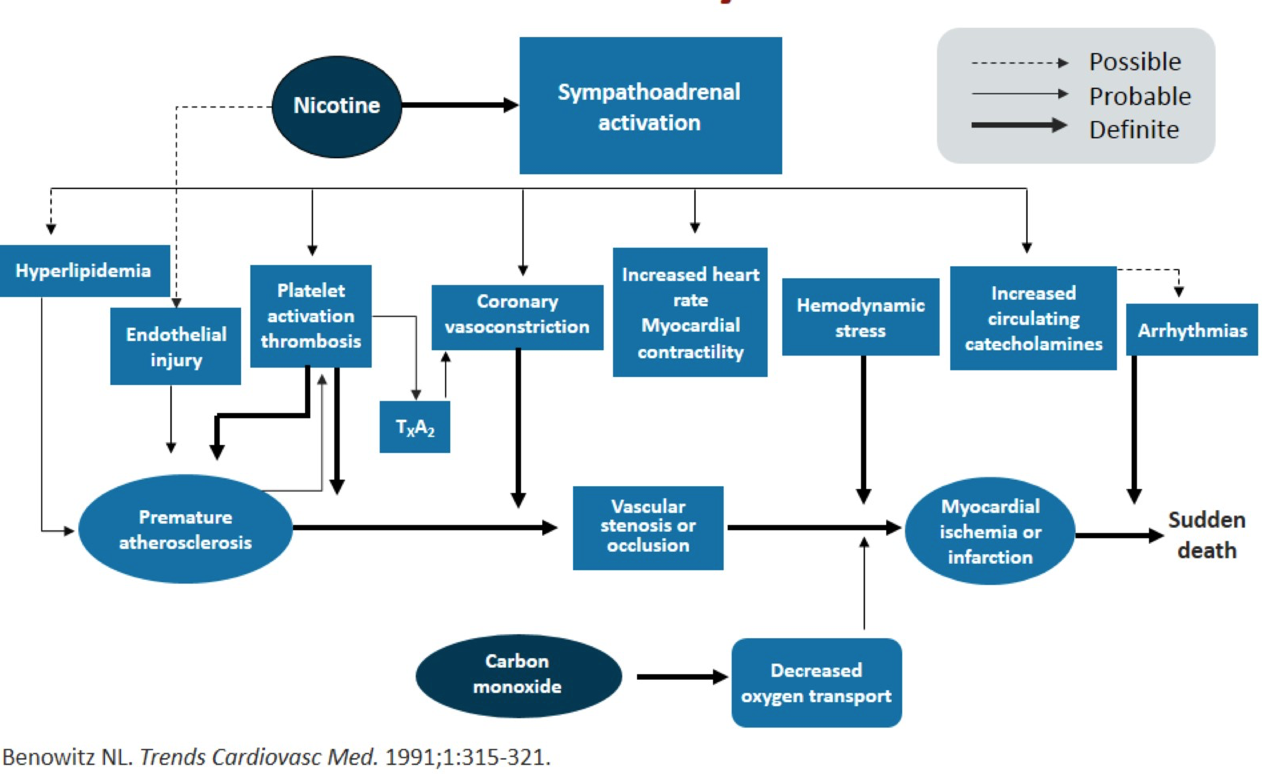
- Note in patients who are <50, smoking is often the only and most important risk factor, with similar prevalence between gender
|
|
|
|
- It is often thought that NRT is contraindicated after a myocardial infarction
- patients with cardiovascular disease were often excluded in the efficacy trials
- From retrospective reviews, NRT does not appear to elicit cardiovascular events in healthy patients, increase risk of first MI or increase 1 year mortality in ACS patients
- Bupropion is well tolerated and safe in ACS patients - there is one small study in outpatients that yielded positive results
- With respect to varenicline, there was a study of 714 patients with stable cardiovascular disease that yielded positive results. verenicline did not increase cardiovascular mortality or all-cause mortality but some cardiovascular events were more common
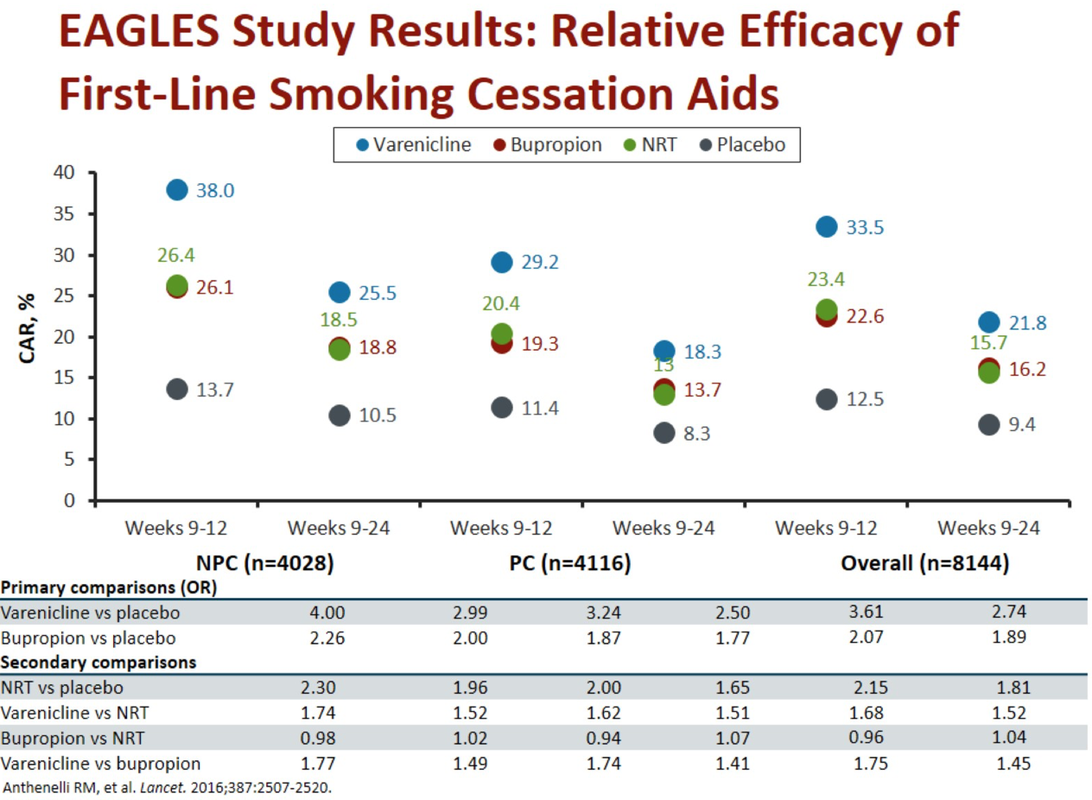
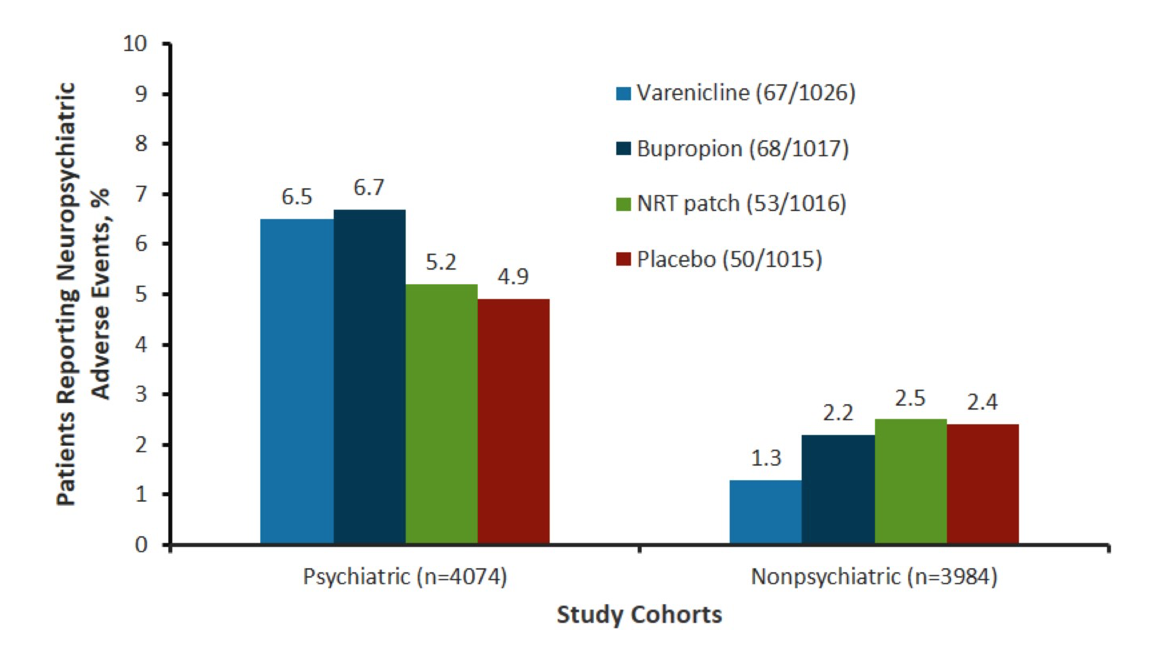
- In terms of neuropsychatric effects - see EAGLES trial published in LANCET 2016.
- Essentially trial was done because neuropsychiatric effects were generalised from post marketing data, observational studies and patients with neuropsychiatric comorbidities were excluded from the study
- There was no increased mod-severe neuropsychiatric effect in either of NRT/ varenicline/ buproprion in people with or without a past/ present history of psychiatric comorbidity.
- There was NO increase in suicidal ideation or behaviour
- This study recruited patients who were STABLE and not unstable
- Buproprion does have medication interactions and can lower the seizure threshold
